Stem Cell Therapy: Promise, Evidence, and Biological Reality
What stem cells can and cannot do — and why the gap between the two matters
This post is for informational purposes only and does not constitute medical advice. Anyone considering stem cell therapy should consult with a qualified healthcare provider familiar with their individual medical situation before making any decisions.
Few areas of modern medicine generate as much hope — or as much confusion — as stem cell therapy.
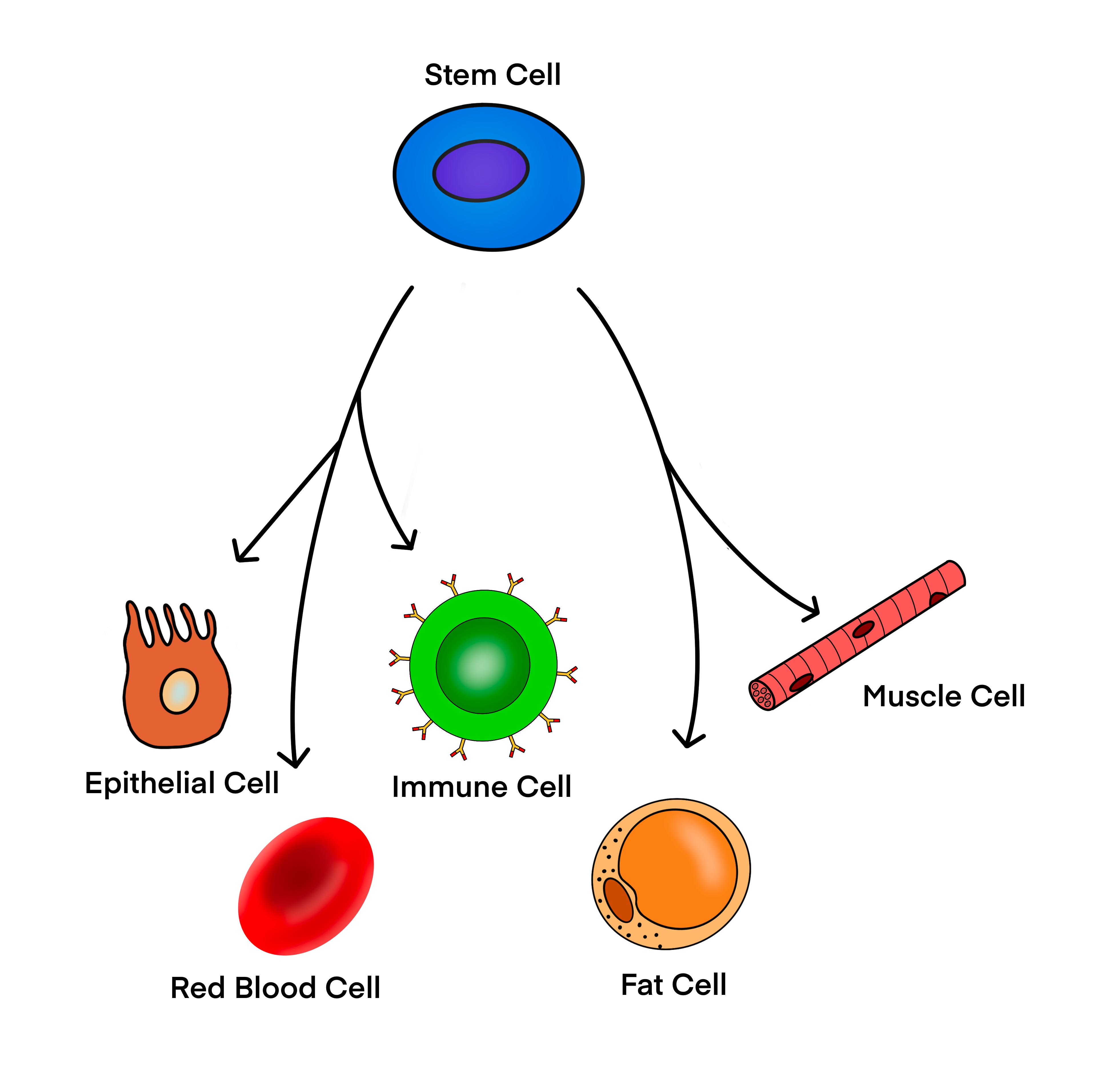
The underlying idea is intuitively powerful. Stem cells can renew themselves and develop into many different cell types. If that capacity could be harnessed and directed, perhaps damaged tissues could be repaired, failing organs restored, and diseases that currently have no treatment reversed.
In some contexts, this is already happening.
In others, it remains a goal rather than a reality.
Understanding the difference requires looking carefully at what the biology actually allows — and where the gap between laboratory promise and clinical application remains wide.
What Stem Cell Therapy Actually Involves
Stem cell therapy, at its core, means introducing cells with regenerative potential into a patient with the goal of restoring function to damaged tissue.
This can take several forms: transplanting stem cells directly, transplanting more specialized cells that were derived from stem cells in the laboratory, using cells to modulate the immune system rather than replace tissue, or growing tissue outside the body and implanting it. The strategies differ, but one biological requirement is constant across all of them.
The cells must survive in a new environment. They must integrate into existing tissue. And they must function correctly once there — without proliferating uncontrollably, triggering immune rejection, or behaving in ways that were not anticipated.
This is where the theory meets the complexity of actual human biology.
Where It Already Works
The most established stem cell therapy is not a recent development.
Hematopoietic stem cell transplantation — bone marrow transplantation — has been used for decades to treat leukemias, lymphomas, and certain bone marrow disorders. After chemotherapy or radiation destroys the patient’s existing blood-forming cells, stem cells capable of rebuilding the entire blood system are infused. Over time, they reconstitute normal blood production.
This therapy works reliably because the biology is unusually well understood. The cell type is defined. The environment it needs to survive in — the bone marrow — is well characterized. The outcome is measurable through blood counts. And the process of integration, while complex, follows predictable rules.
It is, in a meaningful sense, targeted biology. The intervention matches the biology precisely enough that it can be done consistently and safely.
Outside of blood cancers and bone marrow disorders, the picture is more complicated.
Where the Science Is Still Developing
Several other stem cell approaches are in active clinical investigation, with varying degrees of evidence behind them.
Cells derived from pluripotent stem cells — cells capable of becoming almost any cell type in the body — are being tested for retinal disorders, certain neurodegenerative conditions, type 1 diabetes, and cardiac repair. The challenge in each case is not only generating the correct cell type in the laboratory, but ensuring that the cells remain stable, safe, and controllable after they are transplanted into a patient. Cells respond to their environment — to inflammation, to mechanical forces, to oxygen levels, to signaling from neighboring cells. A cell that behaves correctly in a laboratory dish does not automatically behave correctly inside a human body.
A separate class of cells — mesenchymal stem cells — has attracted significant research interest, particularly for inflammatory and degenerative conditions. Interestingly, their effects appear to arise less from directly replacing damaged tissue and more from the signals they release, which can modulate immune responses and support the body’s own repair processes. This shifts the therapeutic model from replacement to regulation — a more subtle mechanism, and one that has proven harder to study rigorously because the preparations vary considerably between studies and manufacturing processes.
Why Translation Is Hard
The distance between a promising laboratory finding and a proven clinical therapy is consistently larger than it appears from the outside.
Demonstrating that stem cells can differentiate into a desired cell type in a dish, or that they reduce damage in an animal model, is an important step. It is not the same as demonstrating that they are safe and effective in humans. Human biology adds layers of complexity that animal models do not fully capture, and the history of medicine contains many treatments that looked compelling in early research and failed when tested more rigorously.
Regulatory agencies require controlled clinical trials — studies designed to detect both benefit and harm — before approving treatments for this reason. The process is slow and expensive. It is also how medicine has learned to distinguish treatments that work from treatments that merely seem like they should.
For stem cell therapies specifically, the requirements are particularly demanding because cells are living entities rather than static drugs. Small differences in how cells are cultured, how many times they have been passaged (i.e., how long they have been grown and transferred to new dishes), how they are stored and delivered, and the biological state of the patient receiving them can all influence outcomes. Demonstrating consistent safety and efficacy across this variability is therefore genuinely challenging.
A Realistic View
Stem cell therapy is not a single intervention. It is a broad category of approaches built on cellular biology, at very different stages of development.
In some settings — particularly hematology — it is well established and life-saving. In others, it is genuinely promising but still experimental, with ongoing trials working to establish whether early results hold up. In a smaller number of areas, treatments are being offered commercially before that evidence exists — a problem covered separately in the post on stem cell tourism.
The biology underlying stem cell research is powerful. Self-renewal and the capacity to differentiate into specialized cell types are real and remarkable properties. But biological potential does not translate automatically into therapeutic success. The path from one to the other requires careful, incremental work — establishing safety, demonstrating efficacy, understanding mechanisms, and following patients over time.
That work is ongoing across many research groups and clinical trials worldwide. Some of it will lead to treatments that change medicine significantly. The honest position is that it is not yet clear which approaches will prove out and on what timeline.
A Note for Patients
If you or someone close to you is considering a stem cell treatment, the most important step is a conversation with a physician who knows your medical history and has no financial interest in any particular clinic or therapy.
Beyond that, it is worth asking whether the specific treatment has been evaluated in controlled clinical trials, whether results have been published in peer-reviewed journals, and whether it is approved by a regulatory body in your country. The International Society for Stem Cell Research (ISSCR) provides a patient handbook and guidance on evaluating specific claims, which can be a useful starting point.
Genuine advances in stem cell therapy are happening. They are happening through the same careful process that all of medicine depends on. That process is worth waiting for.
Background and Further Reading
Copelan EA. Hematopoietic stem-cell transplantation. New England Journal of Medicine. 2006.
Trounson A., McDonald C. Stem cell therapies in clinical trials: progress and challenges. Cell Stem Cell. 2015.
Mason C., Dunnill P. A brief definition of regenerative medicine. Regenerative Medicine. 2008.
Squillaro T. et al. Clinical trials with mesenchymal stem cells: an update. Cell Transplantation. 2016.
Daley GQ. Stem cells and the evolving notion of cellular identity. Philosophical Transactions of the Royal Society B. 2015.
International Society for Stem Cell Research. ISSCR Guidelines for Stem Cell Research and Clinical Translation. 2025. isscr.org